

Posttraumatic stress disorder (PTSD) and substance use disorders (SUD) often co-occur, meaning someone has both disorders at the same time. These people require a more complex course of treatment and have a less favorable outcomes than those with only one disorder. Researchers are actively developing treatments for co-occurring PTSD and SUD, although substantial knowledge gaps still remain in the current research. Integrated psychosocial treatment has the most promising outcome, which includes exposure-based and non-exposure-based treatments. Pharmacologic interventions for co-occurring PTSD and SUD are also under investigation.
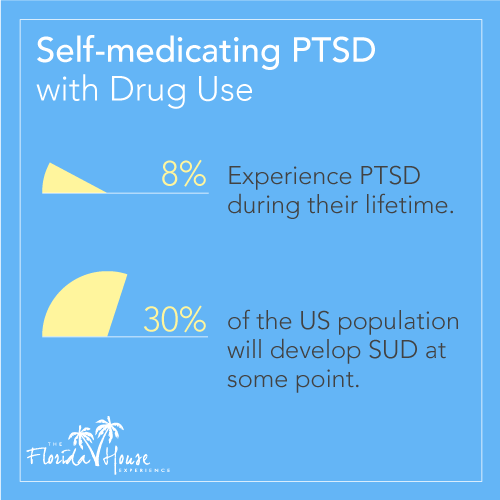 A 2012 study published in International Journal of Methods in Psychiatric Research shows the prevalence of PTSD and drug use. Eight percent of the US population will experience PTSD during their lifetime, and about 30 percent of the US population will develop SUD at some point. This research also shows a strong correlation between the two disorders. Furthermore, individuals with co-occurring PTSD and drug use are at greater risk for other psychiatric problems such as anxiety, depression and neuropsychological impairment. The combination of these conditions creates a complex comorbidity that burdens the healthcare system due to a greater number of treatment episodes, longer duration of these conditions and generally poorer outcomes.
A 2012 study published in International Journal of Methods in Psychiatric Research shows the prevalence of PTSD and drug use. Eight percent of the US population will experience PTSD during their lifetime, and about 30 percent of the US population will develop SUD at some point. This research also shows a strong correlation between the two disorders. Furthermore, individuals with co-occurring PTSD and drug use are at greater risk for other psychiatric problems such as anxiety, depression and neuropsychological impairment. The combination of these conditions creates a complex comorbidity that burdens the healthcare system due to a greater number of treatment episodes, longer duration of these conditions and generally poorer outcomes.
Researchers have proposed several theories to explain the common co-occurrence of PTSD and addiction, but the current empirical evidence provides the greatest support for the self-medication theory. This theory holds that individuals with PTSD have a propensity towards using drugs to mitigate their PTSD symptoms. The greatest support for this theory comes from studies showing that PTSD is typically present before SUD in cases where the two conditions co-occur. Furthermore, studies also show that individuals with co-occurring SUD and PTSD often rationalize their drug use as a means of managing their PTSD symptoms.
Exposure-Based Treatments
Clinicians generally consider exposure-based treatments to be effective for PTSD by itself, but they’re more reluctant to use these methods on patients who also have SUD. This reluctance is mainly due to concerns that exposure-based treatments will increase the risk of drug use during treatment.
 The exposure-based treatments that clinicians use most often for PTSD is Prolonged Exposure (PE), which is a type of cognitive-behavioral therapy specifically modified for PTSD. Some studies of PE include individuals who also have SUD, although the findings on SUD typically aren’t reported or are statistically insignificant. For example, a 2007 study of female veterans published in Journal of the American Medical Association (JAMA) found that PE reduced the symptoms of SUD. However, this study also showed no significant changes in outcomes as compared to the control groups, either in the post-treatment or six-month follow-up examinations.
The exposure-based treatments that clinicians use most often for PTSD is Prolonged Exposure (PE), which is a type of cognitive-behavioral therapy specifically modified for PTSD. Some studies of PE include individuals who also have SUD, although the findings on SUD typically aren’t reported or are statistically insignificant. For example, a 2007 study of female veterans published in Journal of the American Medical Association (JAMA) found that PE reduced the symptoms of SUD. However, this study also showed no significant changes in outcomes as compared to the control groups, either in the post-treatment or six-month follow-up examinations.
Several recent studies have examined the efficacy of integrated plans that combine PE for treating PTSD and a traditional cognitive-behavioral therapy for SUD. Concurrent Treatment of PTSD and Substance Use Disorders using Prolonged Exposure (COPE) is one such plan. It was studied in 2012 as part of a case study on an Iraq veteran with comorbid PTSD and alcohol dependence. Another 2012 study of COPE on Australian civilians found it to be more effective than standard treatments for PTSD and SUD.
Other clinical trials have compared the efficacy of COPE to that of cognitive-relapse prevention among veterans. The preliminary results of these studies show that COPE provides significantly greater reductions in the symptoms of both PTSD and SUD. Furthermore, the reductions in PTSD symptoms accounted for the majority of the variance in the reduction of SUD symptoms, indicating that the drug use in these patients was likely caused by PTSD. More research is needed to determine the efficacy of this approach for different treatment settings.
Non-exposure-Based Treatments
Most studies on the treatment of co-occurring PTSD and SUD have investigated non-exposure-based treatments. A growing body of evidence over the past decade has shown non-exposure-based treatments to be safe and effective to use on patients with co-occurring PTSD and SUD. Seeking Safety (SS) is the most widely used non-exposure-based treatment for PTSD. This therapy consists of 24 sessions that focus on establishing and maintaining safety. The techniques covered in SS include coping with triggers, detaching from emotional pain, setting boundaries in relationships and asking for help. Clinicians also use relapse prevention to treat co-occurring PTSD and SUD, which is a more traditional non-exposure-based therapy.
A 2004 study in The American Journal of Psychiatry compared the results of SS to that of relapse prevention in women with PTSD and SUD. The patients were randomly assigned to a group and given two sessions per week for 12 weeks. No significant differences were observed between the two groups according to the Clinician Administered PTSD Scale (CAPS), which measures the severity of PTSD symptoms.
Pharmacologic Interventions
The use of medication to treat patients with co-occurring PTSD and SUD typically focuses on treating only one of these disorders. Many medications are under investigation, but the medications that have received FDA approval for these purposes is currently limited. For example, the medications approved for alcohol abuse only target relapse prevention. Furthermore, the FDA has only approved selective serotonin reuptake inhibitors (SSRI) for the treatment of PTSD. The Archives of General Psychiatry reports that multiple clinical trials have shown that SSRI therapy achieves PTSD remission for 20 to 30 percent of patients.
Randomized clinical trials have generally failed to show any significant results regarding medications to treat both PTSD and SUD. The most likely explanation for this lack of results is that individuals with SUD are usually excluded from psychopharmacology trials, primarily to ensure patient safety and homogeneity of the study group. Another reason is that a medication has to show efficacy for both disorders independently before it can be considered as treatment for co-occurring PTSD and SUD.
Conclusion
PTSD self-medicating individuals face significant distress and impairment, resulting in a complex clinical course. Substantial gaps remain in the literature regarding the most effective treatment for these people, but integrated psychosocial treatments typically provide the most positive outcomes. Clinicians may also add medication to this therapy, typically after psychosocial treatments are unsuccessful by themselves.
About FHE
FHE Health (FHE) offers a range of services for drug and alcohol addiction, including diagnosis and treatment. Our treatment programs use a long term approach, based on our belief that recovery consists of multiple phases. We implement a medically managed detox, followed by gradually descending levels of rehabilitation. Contact us today to find out more about how we can help you in your journey towards recovery.






